
Understanding Sternocleidomastoid Tumor of Infancy
 When a newborn consistently tilts the head to one side or prefers looking in only one direction, it can worry parents. One common and treatable cause of this condition is Sternomastoid Tumour of Infancy, also known as congenital muscular torticollis.
When a newborn consistently tilts the head to one side or prefers looking in only one direction, it can worry parents. One common and treatable cause of this condition is Sternomastoid Tumour of Infancy, also known as congenital muscular torticollis.
Despite the word “tumour,” this condition is non-cancerous and typically resolves with timely medical care and physiotherapy.
What Is Sternocleidomastoid Tumor of Infancy?
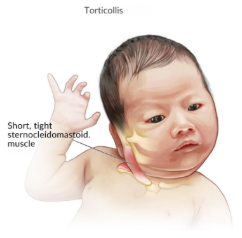 Sternocleidomastoid Tumor of Infancy (SCM tumor) is a benign swelling within the sternocleidomastoid muscle, the large muscle that runs along both sides of the neck.
Sternocleidomastoid Tumor of Infancy (SCM tumor) is a benign swelling within the sternocleidomastoid muscle, the large muscle that runs along both sides of the neck.
The sternocleidomastoid muscle connects:
- The sternum (breast bone)
- The clavicle (collar bone)
- To the mastoid process behind the ear
This muscle helps in:
- Rotating the head
- Tilting the neck
- Supporting head movements
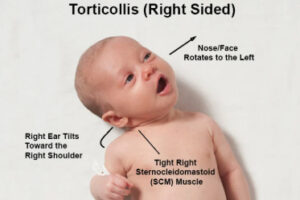
In affected infants, a small, firm lump develops within this muscle — usually noticed between 2–6 weeks of age. Over time, the muscle tightens, causing the baby’s head to tilt toward the affected side and rotate toward the opposite side. This posture is called torticollis.
Why Is It Called a “Tumor”?
The term “tumor” simply means a swelling or mass. In this case, it refers to a localized thickening or fibrosis (scar-like tissue) within the muscle — not a cancerous growth.
Symptoms of Sternomastoid Tumour (Torticollis)
Parents may notice:
Head Tilt
- Baby’s head tilts to one side
- Chin points to the opposite side
Limited Neck Movement
- Difficulty turning head fully in one direction
- Preference for feeding from one breast side
Neck Lump
- Small, firm, non-tender swelling in the neck muscle
- Usually appears within the first month of life
Flat Head
- Flattening of one side of the skull due to persistent head positioning
Facial Asymmetry (if untreated)
- Mild facial imbalance over time
Causes of Sternocleidomastoid Tumor of Infancy
The exact cause is not always clear, but several factors are believed to contribute:
1. Birth Trauma
- Difficult or assisted delivery (forceps or vacuum)
- Prolonged labor
2. Intrauterine Positioning
- Limited space in the womb
- Abnormal fetal position (especially breech presentation)
3. Muscle Injury
- Reduced blood supply to the muscle during birth
- Minor muscle tear leading to fibrosis
4. Large Baby or Multiple Pregnancy
- Increased pressure in the womb
Importantly, it is not caused by infection or malignancy.
Diagnosis
 Early diagnosis plays a crucial role in ensuring complete recovery.
Early diagnosis plays a crucial role in ensuring complete recovery.
Sternomastoid Tumour of Infancy is usually diagnosed through a clinical examination by a pediatrician or pediatric surgeon. Referral to a pediatric surgeon is recommended to confirm the diagnosis and rule out other conditions.
Clinical Examination
A pediatric surgeon will:
- Examine the baby’s neck for a firm, non-tender lump
- Assess head posture and tilt
- Evaluate range of neck movement
- Check for facial asymmetry
- Assess skull shape for positional plagiocephaly
An experienced pediatric surgeon can typically make the diagnosis based on physical findings alone.
Ultrasound (If Required)
If there is any doubt about the diagnosis, the pediatric surgeon may advise an ultrasound of the neck, which:
- Confirms thickening of the sternocleidomastoid muscle
- Rules out other causes of neck swelling (such as cysts or lymph node enlargement)
- Is safe, painless, and radiation-free
Advanced imaging like MRI is rarely needed unless atypical features are present.
Treatment of Sternomastoid Tumour (Torticollis)
The good news: Most cases resolve completely with conservative treatment.
1. Physiotherapy (Main Treatment)
Early intervention (ideally before 3 months of age) gives the best results.
Therapy includes:
- Gentle neck stretching exercises
- Passive range-of-motion exercises
- Positioning techniques
- Tummy time to strengthen neck muscles
Parents are usually taught exercises to perform at home several times daily.
90–95% of infants improve significantly with physiotherapy alone.
2. Positioning Strategies
- Encourage baby to turn head toward the affected side
- Place toys or light sources on the restricted side
- Alternate feeding positions
- Increase supervised tummy time
3. Helmet Therapy (If Plagiocephaly Develops)
If skull flattening occurs and does not improve with positioning, a cranial molding helmet may be recommended.
4. Surgical Treatment (Rare)
Only considered if:
- No improvement after 6–12 months of physiotherapy
- Persistent severe limitation
- Significant facial asymmetry
Surgery involves releasing the tight muscle and is highly successful when required.
Recovery
With early diagnosis and treatment:
- Excellent recovery in most cases
- Full neck movement restored
- Minimal long-term complications
Delayed treatment may result in:
- Persistent head tilt
- Facial asymmetry
- Postural problems
Early intervention is key.
When Should Parents See a Doctor?
Consult a pediatrician if you notice:
- Persistent head tilt
- Baby always looking to one side
- A firm lump in the neck
- Uneven head shape
- Feeding difficulties due to neck stiffness
Early medical assessment ensures faster and complete recovery.
Final Word
Seeing your baby’s head tilted or finding a lump in their neck can be alarming. However, Sternomastoid Tumour of Infancy is a common, manageable condition with an excellent outcome when treated early.
If you suspect torticollis in your child, seek pediatric surgery evaluation promptly — early stretching and positioning can make all the difference in ensuring healthy growth and development.